
The objective of this software is to realize a personalized evaluation of the postural balance to be used in
home-based rehabilitation, by using portable sensors such as Kinect and wii board. After the one time of
identification, the system provide us the personalized estimation of the center of mass (CoM) for the whole
body only with Kinect information, through Statically Equivalent Serial Chain method.
The first function is the adaptive identification interface for the CoM parameters based on Kalman filter
which allows a subject to provide different postures interactively with minimized time length. The second
function is the balance measure visualization (stable or instable) based on the identified model for each subject
considering subject-specific body differences on the segment mass distribution.
Recently, this software was demonstrated at the event of Rencontre Inria-Industrie 13/10/2015 at Bordeaux.
It is also filed at Software Catalogue of Inria.
PersoBalance is registered with the Agency for the Protection of Programs (APP) and deposited at the BNF (Bibliotheque Nationale de France). Its registration number is Antepedia Deposit 20150710154654.
A. Gonzalez, P. Fraisse, M. Hayashibe, « Adaptive Interface for Personalized Center of Mass Self-identification in Home Rehabilitation », IEEE Sensors Journal, vol.15, no.5, pp.2814-2823, 2015. (doi:10.1109/JSEN.2014.2379431)
BalanceGuard: Post-stroke tele-neurorehabilitation using an operant conditioning paradigm under volitionally driven transcutaneous neuromuscular electrical stimulation
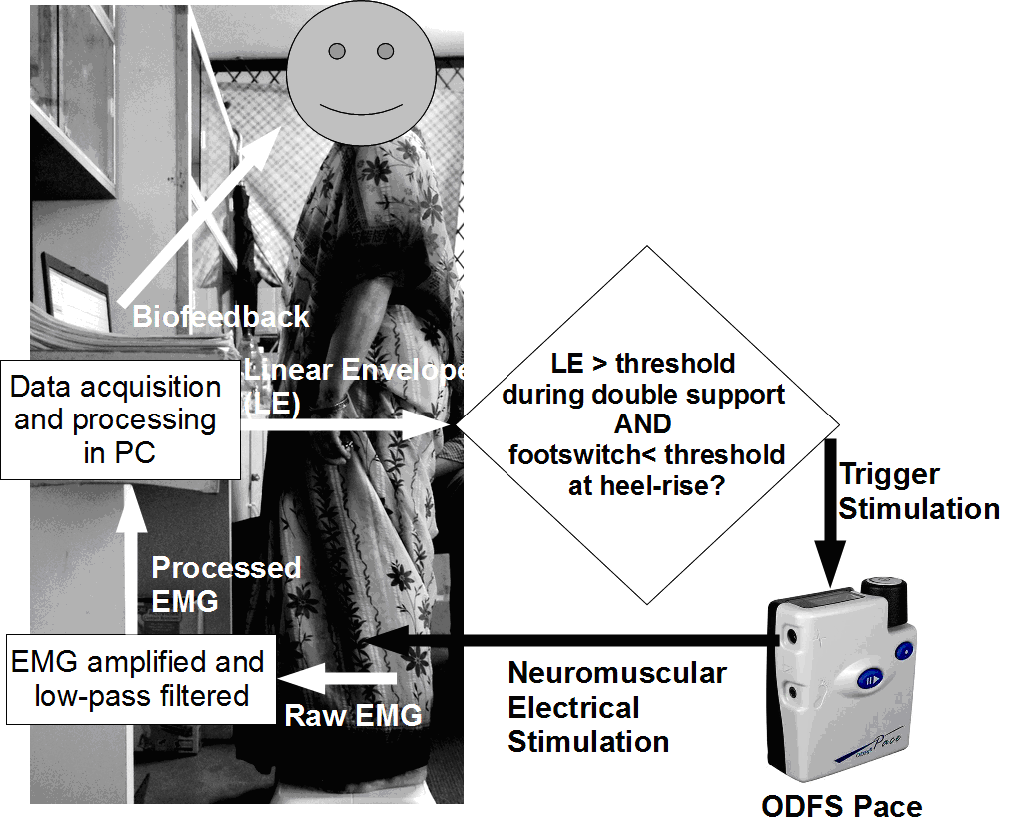
We present a use-inspired neurophysiology-based operant conditioning paradigm that is based on volitionally-driven NMES to generate functional movement for restorative neurorehabilitation. This leads to development and clinical validation of a cyber physical system for teleneurorehabilitation, leveraging the complementary expertise of the project partners from India and France in the work plan with tight integration of the Methods. In addition to short duration visits by researchers, extended visits have been planned to ensure sharing of technology and clinical data collected in India.
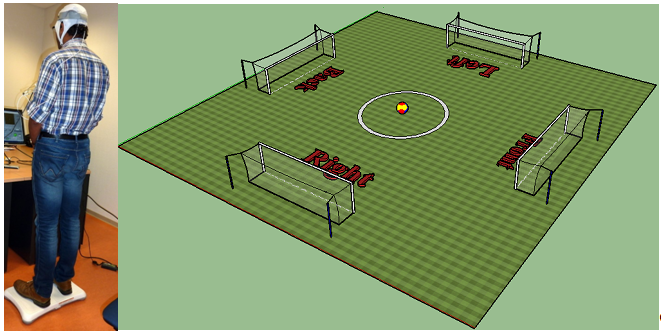
An example of visuomotor balance task which requires the patient to steer the cursor (a ball) to a peripheral target using volitionally generated Center of Pressure (CoP) excursions.
BrainGuard: Development of EEG/EMG-NIRS hardware and software for physiological monitoring during non-invasive electrical stimulation
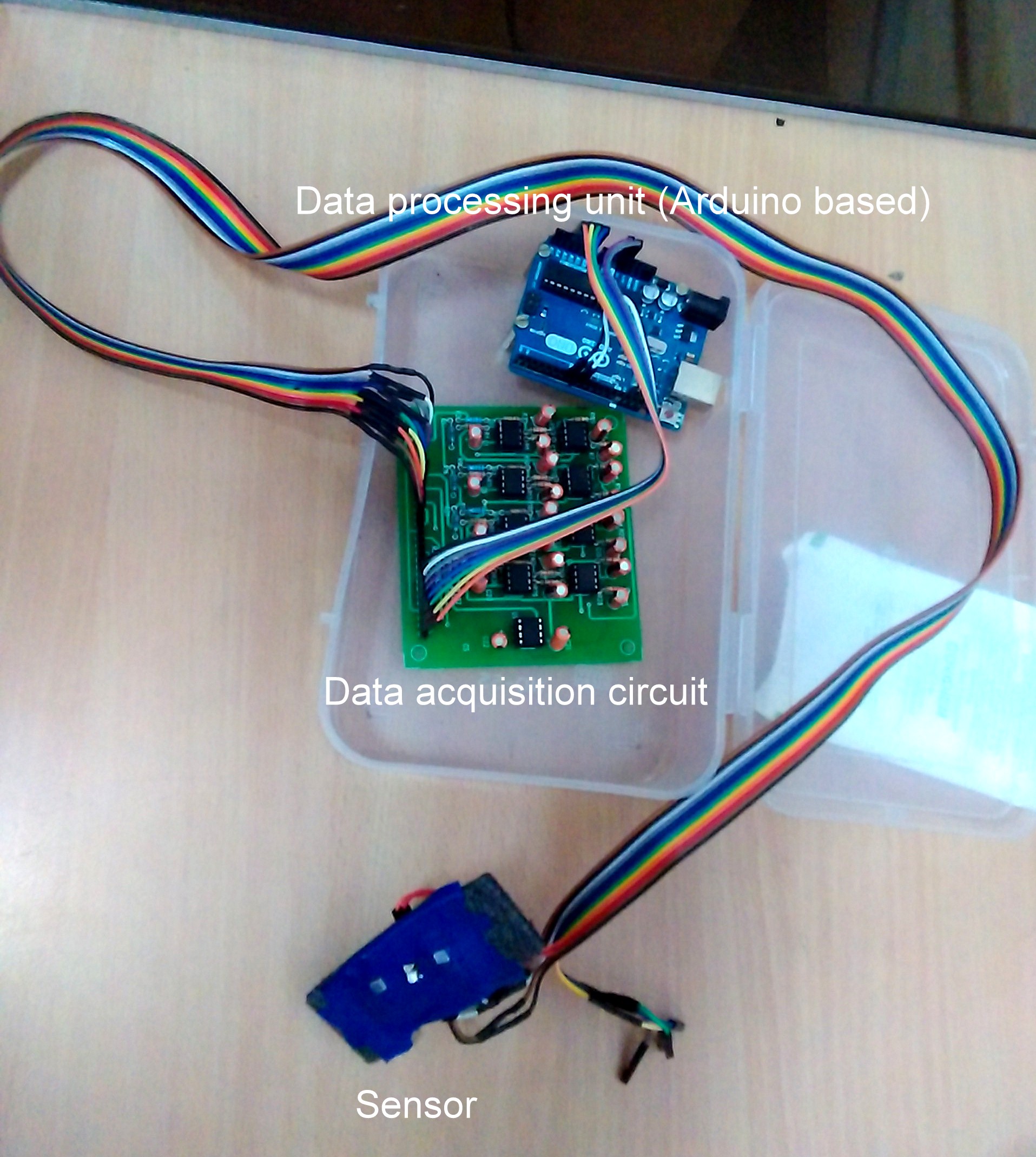
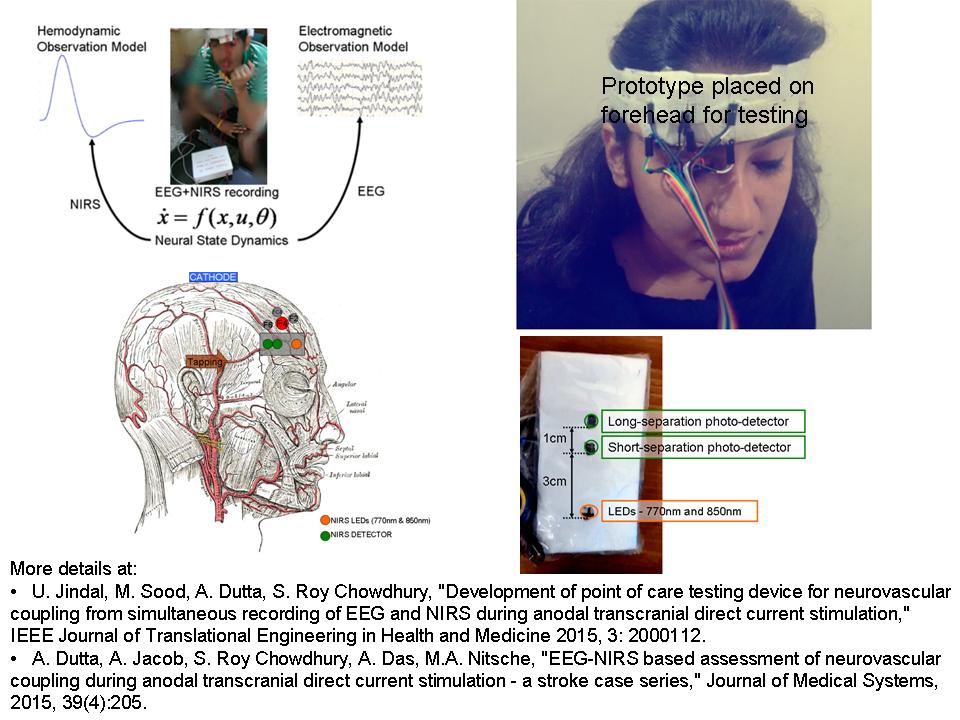
We are developing EEG/EMG-NIRS hardware and software for understanding brain and skeletal muscle physiology during non-invasive electrical stimulation in health and disease. Our objective is to translate this R&D into a low-cost point-of-care-testing device.


NEUROSTIM: EEG/EMG-NIRS guided non-invasive brain stimulation to facilitate neuroplasticity in stroke rehabilitation
The NEUROSTIM project does not only aim to intelligently integrate and interpret data from different neurostimulation and neuroimaging systems: it aims to develop advanced Information Communication Technologies for building an easy-to-use and adjustable neuroimaging/neurostimulation system that patients and health professionals will be able to use and tolerate. Under INRIA, NUMEV and Franco-German PROCOPE funded project, we are currently evaluating the feasibility of offline identification of cortico-cortico and cortico-muscular functional connectivity.
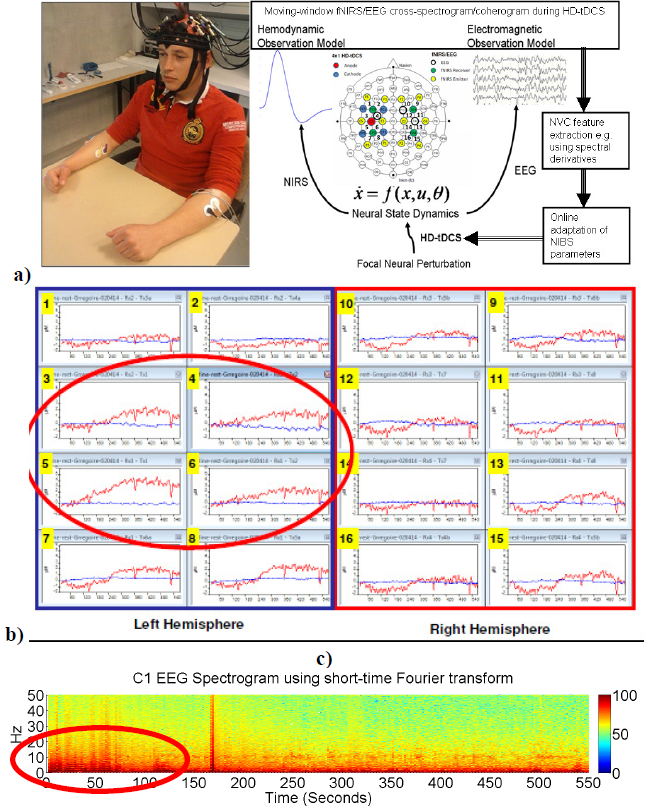
a) Experimental setup of the High Definition (HD)-tDCS and fNIRS/EEG probes/electrodes on the head. An 8-channel dual tDCS-EEG system was used to deliver constant direct current (2mA: 20min) to the left SMC via a 4×1 anodal HD-tDCS electrode montage (anode left SMC (C3) and 4 cathodes as return electrodes). EEG was recorded at 500Hz from all 8 electrodes before and after HD-tDCS (Left: C3, FC1, FC5, CP5, CP1, C1; Right: C4 and FC2), and from 3 electrodes during HD-tDCS (Left: C1: Right: C4, and FC2). A multi channel fNIRS system was used to continually measure at 10 Hz cortical haemodynamic changes from 16 channels covering the bilateral sensorimotor network. Locations of each of the 16 fNIRS channels (Left: 1-8; Right: 9-16) are represented by a receiver-emitter combination. b) Resting-state fNIRS (O2Hb-red traces; HHb-blue traces) during anodal HD-tDCS (2mA) for first ~10 minutes. c) Spectrogram using short-time Fourier transform of the resting-state eyes-open raw EEG at C1 (closest to C3 i.e. anode for HD-tDCS) for first ~10 minutes during anodal HD-tDCS (2mA).
MONISTIS: Facilitating post-stroke neurorehabilitation using neuromuscular electrical stimulation in combination with non-invasive electrical brain stimulation
We also aim to better understand the mechanisms underlying motor control impairments following stroke, including hemiparesis and spasticity, in order to develop novel methods to decrease post-stroke disability. MONISTIS is a binational French-Indian collaborative and translational research project designed to identify brain regions that could serve as hemiparesis and spasticity treatment targets for noninvasive brain stimulation such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). Under INRIA and Franco-German PROCOPE funded project, we are evaluating the feasibility of offline identification of cortico-cortico and cortico-muscular functional connectivity changes under neuromuscular electrical stimulation in combination with non-invasive electrical brain stimulation.
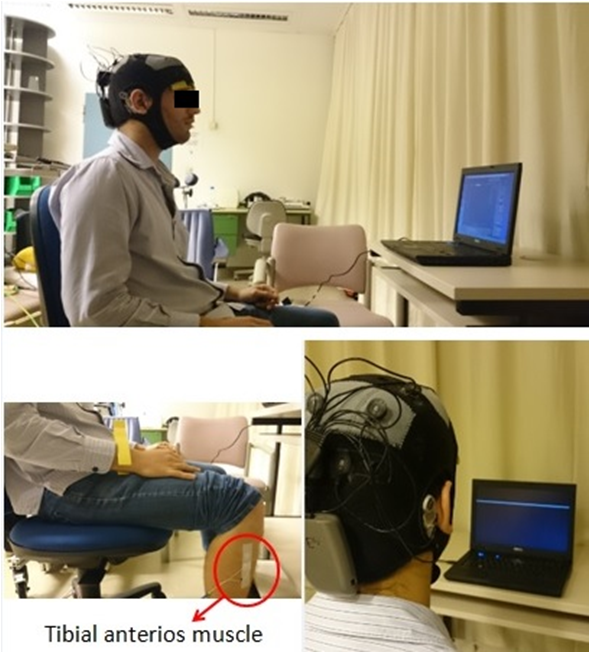
This is a double-blind study where stroke survivors will be randomly allocated to either anodal transcranial DC stimulation (tDCS) or sham stimulation (sham) group. Both the groups will use electromyogram (EMG)-triggered neuromuscular electrical stimulation for gait therapy. The subjects as well as the investigators will be blinded to the application of anodal tDCS or sham intervention.
Investigate time evolution of dynamical quantities, like momenta and inertia, in human motion during non-invasive electrical stimulation-assisted neurorehabilitation using a variable inertia reduced-order model
The proposed research will make use of biomechanics data from healthy and pathological human motion projected onto a novel reduced-order model for gait analysis. This research can also help to relate important dynamical quantities like angular momenta and variable inertias to healthy human and pathological gait at different speeds during non-invasive electrical stimulation-assisted neurorehabilitation.
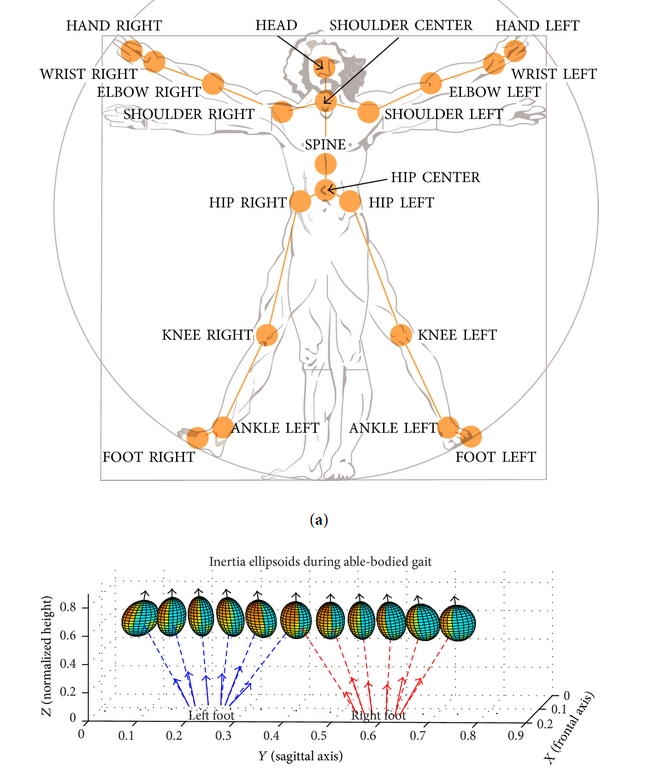
(a) Joint labels for the skeleton model data from Microsoft Kinect. (b) A reduced dimension biped model for capturing the posture. The dimensions of the ellipsoid changes based on the rotational inertia of the body.