Find all our activities in our annual reports here : radar.inria.fr
A parameter optimization method to solve the ECG inverse problem
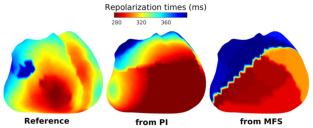
Existing electrocardiographic inverse models express their results either in terms of potentials on the heart surface or in terms of activation times in the heart. G. Ravon developed a new method which gives a potentially more useful answer in terms of three parameters of the underlying action potentials in the heart [1]. Since there are more parameters, care had to be taken to avoid overfitting. Tests on in-silico and ex-vivo data showed good results: the method gave better activation maps than the method of fundamental solutions to which it was compared, and fitted the repolarization phase of the ECG accurately. Figure shows an example of an inversly estimated repolarization map.
 [1] G. Ravon, et al. A Parameter Optimization to Solve the Inverse Problem in Electrocardiography, in: FIMH 2017.
[1] G. Ravon, et al. A Parameter Optimization to Solve the Inverse Problem in Electrocardiography, in: FIMH 2017.
Homogeneous Neumann condition on the torso for solving inverse problems
The electrical activity of the heart creates an electrical field in the body. This phenomenon is classically modelled in a quasistatic manner by Laplace’s equation. The non-invasive electrocardiographic imaging (ECGI) problem consists in retrieving the best electrical map on the heart from given torso measurements. Classically, the solution is found as the best fit between data generated by a forward problem and the actual torso measurements, and it needs a regularization. Hence the inverse solution depends on the matrix of the forward problem, called the transfer matrix, and the choice of the regularization procedure. In 2006, a meshless method based on the method of fundamental solutions (MFS) was adapted by Y. Wang and Y. Rudy [54] to directly solve the inverse problem, combined with a 0-th order Tikhonov regularization. The MFS method is notably more robust than previous methods (e.g. BEM) to the uncertainties introduced by the segmentation of the geometries. In the MFS, the potential is expressed as summation of the fundamental solution of the Laplace equation over a discrete set of virtual point sources placed outside of the domain of interest. The inverse solution is searched as the set of sources that best fit the boundary conditions on the torso, up to the regularization term. This formulation yields a linear system, which matrix depends on the torso and heart geometries, and the boundary conditions at the torso surface. The regularization parameter also heavily depends on the properties of the transfer matrix. The boundary conditions considered in [54] are: i) the Dirichlet conditions, meaning that the potentials at the torso surface are fitted to the recorded ones, ii) homogeneous Neumann conditions (HNC) meaning that the normal flux of current is minimized.
Numerically, the HNC requires to build accurate directions at each measurement location of the body surface, which is a first difficulty. In addition, the body is cut at the top and the bottom where no-flux conditions are probably not relevant. Lastly, the matrix coefficients related to the HNC appears to be much smaller than the ones from the Dirichlet condition, due to the distance between the torso and the actual electrical source (the heart).
J. Chamorro-Servent, Y. Coudière and R. Dubois studied the effect of the HNC on the matrix. They showed that enforcing the Neumann condition has a negligible effect on the solution of the inverse problem. Reconstructed potentials and activation time maps were built for in-silico data. No major differences were found between the standard MFS and the MFS removing the HNC in terms of potentials and activation times. In addition, removing the HNC reduces the ill-conditioning of the problem and the computational burden: the normal at the torso surface is not required anymore, and the problem size is divided by 2. The results of this work were presented as a poster in CinC 2016, and collected in a proceeding for the same conference by J. Chamorro-Servent et al. [18].
Reduced sodium current in the lateral ventricular wall induces J waves in the ECG
“J waves,” a particular abnormal waveform in electrocardiogram (ECG) leads, are associated with a higher risk for ventricular fibrillation. M. Potse has performed a series of simulations to investigate three possible mechanisms that could explain such waves and the associated arrhythmia risk. Out of these, a reduced sodium current in the lateral area of the left ventricular wall turned out to be the most powerful to cause J waves. The lateral area is particular because it is normally late activated, and a further delay due to regionally reduced sodium current can lead to J waves in the ECG. If the same occurs elsewhere in the heart, the resulting J waves would be masked by other ECG peaks. The simulations were supported, as far as possible, by experiments performed at the University of Amsterdam. The results have been published in the journal Frontiers in Physiology, and further refinements have recently been shown in a poster at the Annual workshop of IHU Liryc [14], [43].
Atrial fibrillation due to complex geometry
Atrial fibrillation (AF), a situation in which the electrical activation of the atria proceeds chaotically, is believed to be due to abnormal tissue structure (for example fibrosis), which slows propagation, and abnormalities in ionic currents, which make the action potential shorter. In collaboration with the Center for Computational Medicine in Cardiology in Lugano, Switzerland, we performed series of simulations in which we tried to reproduce these effects [20]. Rapid stimulation of the atria caused AF in some of the simulations, with a likelihood related to the severity of fibrosis. However, we also observed a 30 % likelihood of AF initiation in a model with no fibrosis at all. In these cases, the complex structure of our highly realistic models alone in combination with the rapid-pacing protocol sufficed to create situations of conditional propagation block, which led to a reentrant arrhythmia. These results may shed a new light on the course of new-onset AF. A manuscript on this topic is under preparation.